The first case of COVID-19 in Thailand was reported on 13 January 2020, a female Chinese tourist from Wuhan. It was then widely predicted that Thailand would be the third worst hit by the virus, after China and Hong Kong, largely because of the large number of Chinese tourists, 11 million in 2019. In the first few weeks, before controls were imposed, around a million Chinese may have passed through Thailand.
But today, Thailand accounts for only 0.02% of global deaths from the virus, less than 60 people over almost four months. In the US, more than that number are dying from the virus every hour.
We are going to discuss why the impact has been relatively mild, and what might be the social and economic impact from here onward.
What’s happened: the virus
Two pieces of background information that are important here. First, Thailand has a relatively strong public health system. Its origins date back to the 1970s, when medical students were radicalized in the student movement. Things have changed a lot since then, but a strong commitment to public health was institutionalized in the medical profession. In 2001, public health activists persuaded the government to launch a Universal Health Care system which gave virtually everyone near-free access to health care. Since then there have been attempts to cancel, scale back, or cripple the UHC, but activists have defended it brilliantly. From the late 1970s, activist doctors have also established a network of village health volunteers (O-So-Mo), loosely modelled on China’s barefoot doctors, to extend the reach of primary health care. This network now has about a million people (in a country of 70 million). According to WHO, this unique network played “a crucial role” in tracking and tracing during the SARS epidemic in 2002–3 and bird flu in 2005–6. This public health system has been fundamental to the relative success of managing the virus.
Second, Thailand has returned to military rule after coups in 2006 and 2014, becoming the only country in the world ruled by a government installed by coup. In 2019, an election was held to return to democratic parliamentary rule, but the electoral process was criticized for being non-transparent in multiple ways and ensured that the military clique remained in power. As a result, some people have questioned the government’s legitimacy and its competence.
Through January and February 2020, the spread of the virus was slow. There were probably several reasons for this. First, though medics are reluctant to confirm this, the virus does not seem to like heat and dryness. Through February, Thailand was hot and dry. Second, much of Thailand had been covered with PM2.5 haze for several weeks, meaning that many people were already wearing masks, and the availability of masks was relatively good (there was a shortage only for a short time, maybe a week, as a result of panic buying and hoarding). Third, in treating serious cases of COVID-19, the doctors applied their experience from SARS, including using anti-retrovirals borrowed from HIV-AIDS treatments (perhaps similar to Remdesivir, now being tested on the virus in the US). Fourth, there was probably an element of sheer luck. This virus is very fickle, hitting hard in some places but not in others. Thailand had no hot-spots in this early phase.
Against this background, there was a debate over policy. The medical lobby, which had experience with SARS and bird flu, wanted to impose an early lockdown, following the examples of China, Korea, and Vietnam. But politicians opposed any measures that might injure the economy and, in particular, the huge tourist industry. As such, measures were relatively light—testing people arriving at airports, encouraging people to wash their hands often, and so on.
From the beginning, the public health authorities adopted two critical policies. First, they did contact tracing on every infected case, using both public health officials and the health volunteer network. To give just one example, a Thai returned from Pakistan, passed through the airport tests without showing any symptoms, then died overnight on a train to southern Thailand, and was found to be positive. Within a couple of days, they had traced most of his contacts on the plane, through the airport, and on the train, including people who stood near him on the railway platform, identified from security cameras. Second, they adopted a policy of transparent public information, giving daily accounts of new infections, classified by the source of infection (from abroad, contact with a known case, etc.), and details of each death. The full information was available on websites set up by the Department of Disease Control (See references).
In early March, two hot-spots appeared. The first was at a boxing stadium on 6 March. From this one event, around 150 people were infected. These included a good-looking young actor, whose equally attractive partner was soon also ill. While both survived, their media exposure greatly increased public awareness of the danger of the virus. A second hot-spot appeared in a night-life area. At the same time, there was a growing number of new infections stemming from people crossing the borders, including Thais returning from abroad, visitors to border casinos, and foreigners.
At this point, the government reacted, in somewhat panicky fashion. Between 17-25 March, it closed down Bangkok night-life; imposed a standard lockdown, closing all retail and service businesses except food; imposed a night-time curfew; shut down airports, partially and then completely; and finally passed an emergency law, giving government back the absolute powers it had lost at the 2019 election.
In general, people cooperated. Within days, supermarkets and convenience stores obliged people to wear a mask, have their hands sanitized, and be shot by a temperature gun before admission to the store.
This graph of daily new infections comes from the ministry of public health website, where the data are updated daily. Thailand shows the same pattern as other places that adopted this policy, including Wuhan. After the lockdown, infections continue to rise for 2-3 weeks, then turn downwards. The steepness of the decline depends on the strictness of the lockdown (moderate in the Thai case: no full curfew, partial internal travel restrictions). Now, in the first week of May, seven weeks after the lockdown, daily new infections have dwindled to single figures, and there has been only one death over the past week. The cumulative total of infections is around 3,000, and total deaths is just under 60. The number of infections is certainly undercounted because the testing regime has been passive (see below), but the methodology has been constant, so the shape of the graph is credible. There is no reason to believe the figures have been manipulated.
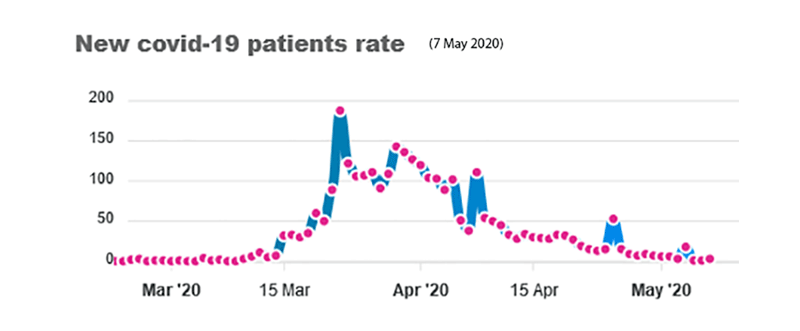
Source: Ministry of Public Health (7 May 2020)
About two-thirds of all cases have been in Greater Bangkok. The other concentrations have been in the tourist resorts of Phuket and Pattaya, and in the far south (especially Yala), where people can cross a very porous border with Malaysia, and from where people have continued to go on pilgrimage. Outside these areas, the numbers of infections have been small.
The Thai strategy has focused on tracing the contacts of known infections. This strategy has one weakness in the case of this stealthy virus: people may be infected, and be capable of passing on the infection to others, while they themselves have minimal or no symptoms. How large the number of asymptomatic carriers may be is a matter of debate. In Iceland, where a 6% sample of the whole population was tested, 43% of those who tested positive had no symptoms (Harmon, 17 April, 2020). Other tests in other countries on smaller samples have found higher proportions of asymptomatic carriers. In early April, a lobby within the Thai public health community predicted that Thailand might have 200,000 or more asymptomatic carriers, and pressed for a more aggressive policy of testing. The policy-makers argued that this method was unnecessary and expensive, and that test kits were hard to come by. But in Vietnam, a country comparable to Thailand in many ways, the authorities had adopted a policy of pro-active testing from late January, including developing domestic production of kits and smartphone contact apps, and claimed to have a record of zero deaths from the virus.
Around 12 April, the local public health authorities in Phuket began more pro-active testing. By the end of the month, the central authority also changed policy, and announced it had begun “active case finding,” which meant identifying at-risk segments for conducting random tests, and had also commissioned a local firm (Zenostic) to produce test kits. The target segments included people crossing the southern border, migrant labor (especially after the experience of Singapore), and prisoners. From 1997, the public health authorities had developed a branch of the health volunteer network to cover the large (2-3 million) migrant population, largely from Myanmar, and had used this network to ensure that migrants were educated about the dangers of the virus and cooperated in tracing.
What’s next: the impact
Even though the epidemic has been relatively mild compared to many other countries, the economic and social impact will be heavy and long-lasting, simply because the Thai economy is so exposed to the outside world. Exports were 67% of GDP in 2018, and 40 million tourists visited in 2019.
The Thai central bank predicted the economy would shrink -5.3% in 2020, and the IMF raised this to -6.7%. Both estimates are probably over-optimistic. The nearest guide to the possible impact is the Asian Financial Crisis of 1997-8, which began in Thailand and was severest here; the Thai economy shrank by 14% over 18 months; two million people in the formal economy were immediately made unemployed, and many more in the informal economy lost their livelihood; thousands of businesses went bankrupt; and five percent of households dropped below the poverty line.
But four factors softened the impact in 1997/8. First, the traditional social safety net provided by family, community, and village worked rather well. Millions of people left urban areas and returned to a rural origin. Most of them were first-generation migrants, and still had good claims on the support of family and community. Second, because Thailand is a food surplus community, almost none faced starvation as a part of severe distress. Third, government delivered relief, in the form of grant aid and micro-credit, direct to local communities, in order to avoid the delay and leakage of working through the bureaucracy. Fourth, because the crisis was confined to Asia, the rest of the world pulled Thailand and other countries out of the crisis relatively quickly. When prices fell, exports increased, and people arrived to have a cheap holiday or buy up a bankrupt business at bargain prices.
This time will be very different. Firstly, over the two decades since the Asian Crisis, the urban population has greatly increased, maybe doubled. Many more of the workforce are more distanced from a rural origin: they were perhaps born in an urban area, and have less access to the traditional social safety net. Secondly, Thailand is entering the second year of an El Nino drought. Though the drought appears less severe than earlier predicted, people who have returned to a rural home and begun planting rice have been warned that there may not be enough water to bring the crop to harvest. Thirdly, this government is centralized, bureaucratic, and top down-minded. And finally, the rest of the world will not help to pull Thailand out of the crisis, but in fact will make it worse. The mismanagement of the virus in the US, UK and elsewhere will ensure that the damage to the global economy is deeper and more long-lasting. Demand has plummeted. Global supply chains are breaking down. Shipping companies and airlines face bankruptcy. Tourists will not be returning soon.
The kind of lockdown implemented in Thailand on March 26 has a very heavy impact on the economy, and especially on the urban informal sector—small shops and service businesses, vendors, casual and day labor. Something like 13-15 million may have immediately lost their livelihood. There has also been a heavy impact on farmers who produce goods such as fruit for export. Exports have been disrupted, and prices have dropped steeply.
The two-fifths of total households at the bottom of the income pyramid have negative savings, meaning they have no savings or are already in debt. So, the loss of income will mean immediate distress. Within days of the lockdown, long lines appeared at organizations offering aid, especially food. The government has probably not had any involvement in distributing food since the Second World War.
While Thailand has excelled in constructing a public health system, other forms of social security are very weak. In the early 2000s, government made some beginnings, but the subsequent military governments have favored targeted, discretionary systems which depend on identifying those in need.
Soon after the lockdown, government offered monthly handouts of Baht 5000 (approximately US$ 170) for three months to households that could prove they had lost their employment or livelihood. On the day the scheme opened, 20 million people attempted to apply, crashing the application website. The government announced that only 9 million qualified for the handout (and at one point reduced the scheme to a single month, but had to renege), causing widespread anger. Many from the informal sector face difficulty providing the required proof of loss of livelihood, and handling the electronic application system. Government allowed those rejected to appeal. Other provisions in the package included a moratorium on debts to state institutions, and support for SMEs. Subsequently, the government added a handout to farmers. Around a million formal-sector workers qualified for emergency unemployment benefit under the Social Security Scheme, but over half were told to wait because the computer system failed.
In the short term, the government has no real difficulty in financing rescue schemes. It has called back low-priority allocations from all the ministries, and the debt-to-GDP ratio (at 42% before the crisis) is projected to remain below the 60% ceiling. However, the government’s current economic team was recruited to boost economic growth. They may not be the right people to manage the social consequences of an unprecedented economic slump.
From the beginning of May 2020, government has begun to ease the lockdown, first by allowing small shops and businesses to begin operation, while laying down rules to ensure that social distancing is maintained. It promises a cautious, phased opening of other concerns.
There is, however, no sign yet of a strategy to manage the longer-term slowdown stemming from the global crisis. China is likely to be the first major economy to revive, and this will have a positive effect on the Thai economy, though will pose some political difficulties. The larger question is whether the remaking of the world economy by the COVID-19 crisis will render obsolete the strategy followed by the Thai economy for the past four decades (exports, FDI, tourism). If the major economies bring more manufacturing home, institutional investors concentrate more on their domestic markets, and tourists venture less far afield, Thailand’s old sources of growth will disappear.
Already before the COVID-19 crisis there was debate on the soundness of the government economic strategies of continuing to promote tourism and FDI in high tech industries, given that Thailand’s growth rates had been lower than ASEAN neighbors for about a decade. Countries like Vietnam and Indonesia have become more attractive to foreign investors because of their younger labor force, larger markets, and more stable politics. Critics also pointed to the impact of the open strategy on the environment, and the failure to resolve Thailand’s inequalities in income and wealth. Dissident economists argue that Thailand needs policies which cultivate local sources of growth by reducing monopolies, reforming the tax system, shifting power away from the center, improving social welfare programs, enhancing the quality of education, and confronting global warming, which is already causing higher incidence of droughts and floods.
Some conclusions
In Europe, the health services are being rightly cheered for their work during this crisis. In Thailand, they deserve the same applause but are not getting it, because their work is in the past or in the background, not in front of the TV cameras. Two key factors account for the relative mildness of the outbreak: first, the efforts of medical activists, extending over half a century, to create a public health system with universal coverage and with exceptional reach due to the network of health volunteers; and second, the qualified success of the medical lobby in negotiating with politicians over policy.
However, the economic and social impact is another matter. We are in uncharted territory. The disruption of the global economy is on a scale not seen since the Great Depression and Second World War. How societies will react is impossible to predict. There is strong possibility that government in Thailand, as elsewhere, will seize this opportunity to strengthen authoritarian rule and minimize changes to the status quo. But big crises are also big opportunities to achieve major shifts in policy.
8 May, 2020
References
- Department of Disease Control. 2020. Corona virus disease (COVID-19) ddc.moph.go.th/viralpneumonia/eng/index.php. (Accessed 3-7 May 2020)
- Department of Disease Control. 2020. COVID-19 Infected situation reports. https://covid19.th-stat.com/en. (Accessed 3-7 May 2020)
- Harmon, Amy. 17 April, 2020. Why We Don’t Know the True Death Rate for Covid-19. New York Times. https://www.nytimes.com/2020/04/17/us/coronavirus-death-rate.html. (Accessed 7 May 2020)
- Somruedi Banchongduang. 26 March, 2020. BoT predicts 5.3% GDP dive in 2020. Bangkok Post. https://www.bangkokpost.com/business/1886495/bot-predicts-5-3-gdp-dive-in-2020. (Accessed May 7 2020)
Pasuk Phongpaichit is Professor of Economics at Chulalongkorn University, Bangkok. Chris Baker is a historian. Together they have written widely on Thailand’s political economy, history, and culture. In 2017 they jointly won the Fukuoka Grand Prize.
Citation
Pasuk Phongpaichit and Chris Baker. 2020. “Thailand and COVID-19: What’s Happened and What’s Next” CSEAS NEWSLETTER, 78: TBC.